Dr. Gerald H. Smith
Many advances have been forthcoming since Dr. William Sutherland discovered cranial motion in 1939. Because of his pioneering efforts, osteopathic and chiropractic physicians have achieved many miraculous results utilizing craniopathic principles. In recent years, widespread publication of craniopathy, has stimulated a grass roots interest within the dental profession.
Cranial bone motion does exist and at present there are documented references(1,2,3,4,5,6) pointing to this fact. The significance of this discovery goes far beyond the mere fact that these bones move. Cranial motion represents part of the craniosacral respiratory mechanism. The inherent motion of the central nervous system is transmitted via the cerebrospinal fluid to the dural membranes, which in turn control and influence the cranial bones and sacrum. The function of this primary respiratory mechanism underlies the essence of life itself.
For years, TMJ specialists, osteopaths and craniopaths have recognized the need to maintain cranial bone motion when restoring the dentition. Because of men like Al Fonder, Hal Ravins, Carl Mestman, Willie May, Justine Jones, Stephen Smith and others many of the conventional dental concepts are being challenged. Physiologic dentists are concentrating their efforts on educating the health profession of the far reaching structural and neurologic consequences that conventional techniques have and their disruptive effects on the cranio-sacral primary respiratory mechanism.
Conventional dental techniques restrict cranial bone motion by crossing the maxillary mid-line with fixed bridgework. Because the maxilla articulates the nine other cranial bones (malar, frontal ethmoid, vomer, palatine, lacrimal, sphenoid, inferior nasal concha and other half of the maxilla) it represents direct contact with 45% of the cranium. In essence, locking the maxillae will restrict to varying degrees the entire craniosacral mechanism. Since each patient’s physiologic adaptive range varies, the clinical extent of their symptoms will ultimately depend on their levels of distress. Patient complaints of severe headaches, facial pain, chronic fatigue, mental confusion, eye pains, irritability, disequilibrium and many more seemingly unrelated symptoms have been resolved once the mid-line restriction was removed and cranial rhythm re-established.
Case Report
A 42 year old white female was referred to the author for evaluation of numerous chronic symptoms. The dental history revealed extensive fixed bridgework fabricated by a board certified prosthodontist.(7) The patient’s symptoms commenced after cementation of fourteen units of maxillary fixed bridgework. Some symptoms appeared immediately upon bridge placement while others were progressive. The permanent bridgework was placed fourteen months prior to the evaluation and the patient ran a high fever for days after the procedure. The following chief complaints were presented by the patient.
- Constant hat band headache – immediate
- Facial and cranial tightness – immediate
- Generalized feeling of stress and irritability – immediate
- Upper cervical neck pains – immediate
- Limited right and left rotation of the head – immediate
- Disequilibrium – progressive
- Generalized chronic fatigue – progressive
- Generalized muscle weakness – progressive
- Paresthesia of the arms and legs – progressive
Examination and Diagnosis
On physical examination, the patient was found to be an apparently healthy, cooperative and alert individual. Her present medical history was unremarkable. Past medical history revealed surgical removal of the right ovary, appendectomy and in 1982 a lumpectomy on the right breast was performed. A review of her systems showed them to be essentially normal. A hematologic profile (SMA 12) revealed all values to be within normal limits with the exception of phosphorous(4,7).
Palpation of the following cranial sutural areas elicited tenderness:
- R&L Sphenotemporal
- R&L Occipito mastoid
- R&L Lambdoidal*
- R&L Zygomatico malar*
- R&L Maxillomalar*
- R&L Frontomalar
* A gentle force applied to these sutural areas brought temporary relief from the constant head pressure.
Rotation of the head exhibited a definite restriction of approximately 45 degrees to both the right and left.
Audiometric(8) testing revealed a 20 decibel loss in the 125, 250 frequency range. This signified an impedience of the middle ear ossicles.
Cinefluorosopic motion studies(9) revealed a definite restriction of movement of the atlas-axis primarily in flexion-extension and to a lesser degree in rotation and sidebending.
A diagnosis of restriction of cranial bone motion and cranial dural membrane torquing was made on the basis of:
- Palpatory restricted ranges of cranial bone motion.
- Restricted motion of the atlas-axis complex as depicted by cinefluoroscopic radiography.
- Immediate appearance of severe clinical symptoms and relative short duration of appearance of the progressive symptoms after the fixed bridgework was placed.
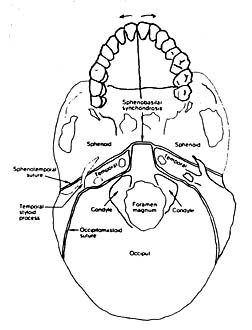
Figure 1 – The mid-palatine (cruciate) suture permits the two halves of the maxillae to move into external and internal rotation. This micro-motion translates to a horizontal separation movement between the maxillary central incisors. Splinting these two teeth by means of fixed crowns effectively restricts the cranio-sacral respiratory mechanism.
Treatment
Emergency treatment was rendered by cutting the maxillary mid-line connection between the central incisor crowns. Immediate relief was felt as soon as the cast connection was separated. The hatband headache, facial and cranial tightness, restriction of head rotation, upper cervical pain and cranial stress disappeared immediately. Within days the paresthesia to the arms and legs diminished to the point where only a slight residual effect remained in the right arm. In approximately two weeks, the remaining symptoms resolved: disequilibrium, chronic fatigue and muscle weakness.
Audiometric tests performed after the bridgework was separated revealed an increase of 20 decibels in the 125 and 250 frequency range. Post treatment cinefluoroscopic radiography revealed an increase in flexion-extension rotation and side bending movements of the head.
Final restoration of this case will require the use of a new design of physiologic precision attachment – CMA 1284™. This attachment involves a piston-cylinder arrangement which is totally esthetic and is incorporated within the adjacent two central incisor teeth. The device enables “splinting” of the front bridgework and simultaneously permits motion for the maxillary bones.
Discussion
The question of whether or not cranial bone motion exists is no longer an issue. The issue now is how not to violate this physiologic motion when restoring the dentition. This author’s recent findings, plus other personal clinical experiences as well as similar encounters of other dentists throughout the country support the concept that the maxillae must not be restricted. Although not every patient with a maxillary partial denture or anterior fixed bridgework has clinical symptoms, a compensatory response must exist somewhere in the system. For every action there is a reaction, and man’s ability to adapt within a physiologic range is his means of survival. Cranial restrictions can have far reaching neurological effects as well as influence flow of the cerebrospinal fluid, dural membrane torque and its influence on the vertebrae, sacrum and physiology of the body.
Acute and chronically ill patients with seemingly unrelated symptoms must now be evaluated dentally. Such an evaluation may prove invaluable and offer a non-invasive approach to health.
References
- Fryman, Viola M: “A Study of the Rhythmic Motions of the Living Cranium,” Journal of the American Osteopathic Association, Vol. 70, No. 9, May 1971.
- Michael, David K and Retzlaff, Ernest W: “A Preliminary Study of the Cranial Bone Movement in the Squirrel Monkey, The Journal of the American Osteopathic Association, Vol. 74, May 1975.
- Retzlaff, Ernest W et al: “Cranial Bone Mobility,” The Journal of the American Osteopathic Association, Vol. 74, May 1975.
- Tettambel, Melicien, et al: “Recording of the Cranial Rhythmic Impulse,” The Journal of the American Osteopathic Association, Oct. 1978.
- Greenman, Philip E: “Roentgen Findings in the Craniosacral Mechanism,” Journal of the American Osteopathic Association, Vol. 70, Sept. 1970.
- Baker, Ernest G: “Alteration in Width of Maxillary Arch and Its Relation to Sutural Movement of Cranial Bones,” Journal of the American Osteopathic Association, Vol 70, No. 6, Feb. 1971.
- Thomas Balchi, D.D.S., 1244 Fort Washington Ave., Fort Washington, PA 19034
- Richard Bevans, Audiologist, Court & Centr Ave., Newtown, PA 18940.
- Edward Blumenthal, D.C., 444 North York Rd., Hatboro, PA 19040.
- Arno Burnier, D.C., referring chiropractor: 81 South Main Street, Yardley, PA 19067.
