Dental / Facial Pain / Posture Connection
Enduring ten plus years of facial pain diminishes one’s quality of life. The real frustration comes from consultations with many medical and dental specialists with no results.
Thinking out side of the box is key to resolving problems that do not respond to treatment with in a three to six month period. Unfortunately there are many potential sources for causing pain: viral and bacterial infections, loss of nerve integrity, nerve compression and entrapment within spastic muscles, jammed cranial sutures, referred pain of dental origin, tension within the dural membranes, tumors, and structural distortions from below (pelvic, sacrum, leg or foot imbalances). In my clinical experience most chronic facial pain issues come from structural dental cranial distortions. This was the case with Noreen T.
Most people have malocclusions or bad bites. As a result of abnormal tooth contact the muscles, spine, pelvis and feet can become distorted. An integration of many different specialties is required to understand the functional anatomy and how different parts of the body relate to one another. Without this knowledge, practitioners cannot begin to look for the underlying causes of structural pain.
When a patient’s bite if off, the chewing muscles are in a state of tension. All it takes is an episode of additional stress or physical activity to upset the balance. With patients who have multiple structural imbalances, once the spasm starts it is more difficult to self-correct and their pain lingers. Spastic muscles place tension on the skull sutures. A jammed suture can cause pain from compression of the vital structures (blood vessels, lymphatics and nerves and connective tissue). In addition, nerves traversing through or in close proximity to the muscle get stimulated. Balancing the cranial bones and placement of a dental “shim” or “shims” is often required to rebalance the system and resolve the pain.
Noreen T. presented with cranial distortions that immediately corrected when a paper shim was placed between the appropriate teeth coupling. It was also of interest that Noreen exhibited pronation of her feet. Foot pronation can either be an ascending lesion causing structural distortions up the spine or a descending lesion coming from dental cranial distortions affecting the feet. Treatment consisted of a cranial adjustment and placement of a resin “shim.” The entire procedure took 90 minutes and Noreen’s 10-year facial pain totally disappeared. The key to structural correction is to define the specific strain pattern and determine what will take it out. The direct connection between the dental/cranial complex and the feet is the dural tube, which surrounds the brain travels down the spinal cord and attaches to the second sacral tubercle. Distortions of the sacrum will influence pelvic posture and ultimately the position of the legs and feet, which have to compensate.
Figure 1.
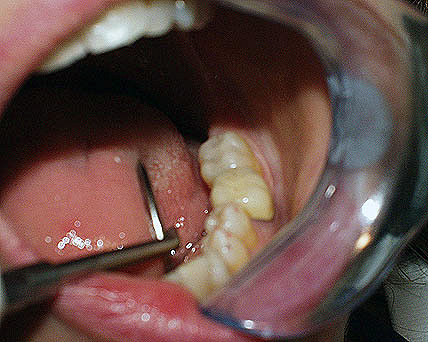
A resin “shim” the thickness of one sheet of typing paper was placed on the lower second molar. This thin support was essential to remove the strain pattern from the patient’s skull, sutures and dural membrane system.
Figure 2.

Bilateral pronation. Pronated feet can be caused from weak ligaments or lack of muscle support for the arch. Pronation and/or flat feet are usually associated with weak adrenal glands. Under active adrenals are associated with low levels of vitamin C (weak ligaments) and a weak posterior tibilais muscle, which helps support the arch of the foot.
The left foot was worse than the right. Pre-treatment photo was done before a cranial adjustment and placement of the supporting “shim” was done.
Figure 3.

Pronation of the feet dramatically changed immediately following treatment: cranial adjustment and placement of a “shim”. This documents that the cranial/dental distortion was a descending lesion that caused the foot pronation. Use of a Rothbart proprioceptive stimulator is a future option.
Figure 4.
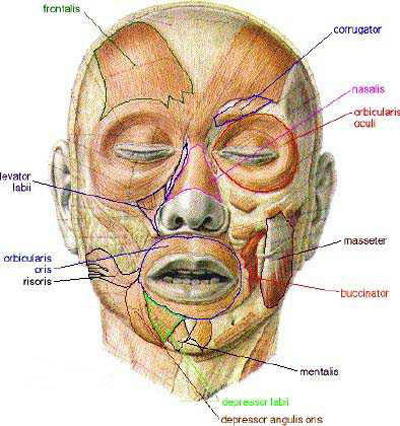
When the bite is off and the cranial bones are not balanced, the facial musculature is out of balance. This results in facial spasm and pain.
Figure 5.
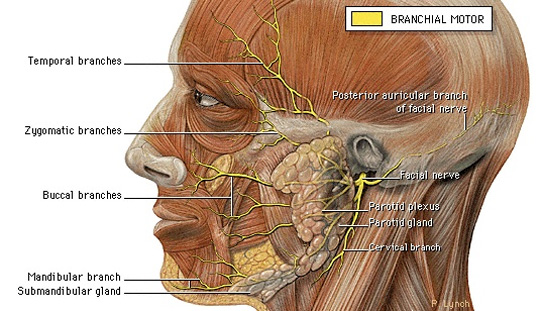
The anatomical location of the seventh cranial or facial nerve (noted in yellow) defined the exact location of Noreen’s ten-year facial pain pattern. One should note that the facial nerve lies directly on the masseter muscle, which is one of the primary chewing muscles.
Distortions of the sacrum will influence pelvic posture and ultimately the position of the legs and feet, which have to compensate.
FREE PRESENTATION
Download the slides from Dr. Smith's presentation on the Dental Whole Body Connection in Ontario on October 25, 2024.
A comprehensive seminar to awaken you to the potential dangers of dental treatments.

STAY INFORMED
Big tech and mainstream media try to suppress the powerful information I have to share. Subscribe here to stay informed!