Facial Pain / Dental Connection
JM suffered with facial pain for twenty-two years despite extensive medical, dental, chiropractic evaluations and even surgical intervention. JM’s saga began in her twenties, when she had seventeen crowns fabricated to restore her posterior teeth. The dentist who performed the restorations was competent from a mechanical perspective, that is, the anatomical crown forms, porcelain shade and marginal fit all fell within the standard of care as defined by the dental schools. Unfortunately the dental schools, both in the past and present, have not discovered the functional link between the teeth and the craniosacral system. There is a delicate balance between the meshing of the teeth and stability of the twenty-eight skull bones. Not only do the teeth rebalance the cranium but also maintains balance of the muscles, ligaments, cervical vertebrae and pelvis. The functional link that ties the entire system is a membrane system, the dural tube, which surrounds the brain, passes out the base of the skull, attaches to the upper three cervical vertebrae and continues down to the second sacral tubercle. This reciprocal system functions like a slinky and any distortion from above can effect changes below and vise versa.
Reconstructing a patient’s teeth involves a high skill level. Not only must the dentist possess the abilities to prepare the teeth properly, make good temporary crowns, take accurate bite registrations and impressions but equally important is his ability to adjust the biting surfaces of the crowns to balance the skull bones when the teeth come together. This latter task is not taught in the dental schools and is only learned in post-graduate courses. The integrated concept is not taught as a unified package. Osteopaths and chiropractors that specialize in cranial concepts teach the basics of the cranial mechanism. Most dentists are unaware of the existence of this knowledge base. Only through studying both functional dental orthopedics as it relates to the cranium and the cranial mechanism as it relates to dental structures can one begin to recognize how closely knit these two specialties really are. Unfortunately there are very few dental practitioners who have mastered integrating these two fields and capable of providing this type of service.
JM had undergone sinus surgery in an attempt to resolve the facial pain. The ENT specialist made a diagnosis of sinusitis and believed it to be the underlying cause of the patient’s problem. Reality soon set in when the post-surgery did not produce the anticipated results. The cause of the chronic facial pain was the inaccurate contact made by the posterior crowns. Improper contact resulted in jamming sutures between skull bones as well as tension placed on the dural membranes within the skull. Treatment involved manually manipulating the skull and judiciously adjusting the bite. The process took four months to complete. The facial pain of twenty-two years resolved.

Figure 1
The posterior crowns had biting interferences, which caused jamming of cranial sutures, and placed strain patterns within the patient’s skull.
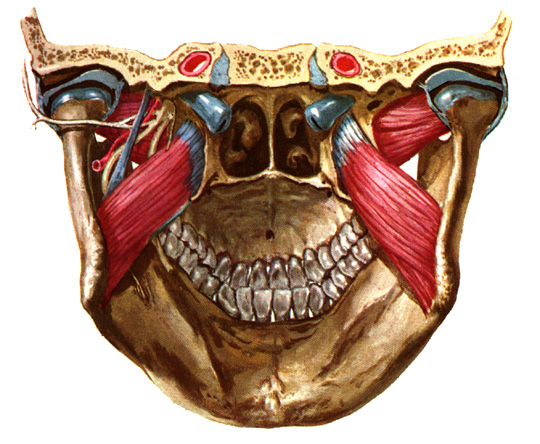
Figure 2 (above)
An ideal occlusion or balanced bite provides even pressure to the skull bones and balances the muscles and ligaments. The upper teeth are set in the maxillae, which represents the anterior two-thirds of the cranial base. If the upper component is distorted (crooked teeth, one side higher than the other) then the forces generated by the teeth will distort the skull. In addition, bite interferences often trigger off muscle spasm, which in turn can jam sutures and distort cranial bone alignment. One of the principal functions of a balanced bite is to serve as a self-correcting mechanism for rebalancing the skull. This rebalancing occurs every time one swallows which is two to three times per minute.
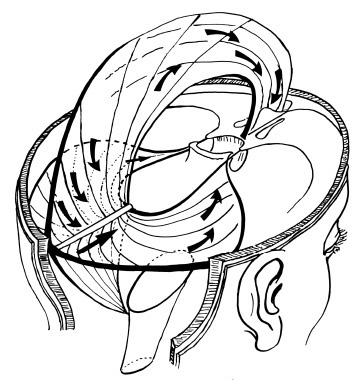
Figure 3 – Referred Pain Patterns (above)
“… tugging on the venous sinuses, damaging the tentorium, or stretching the dura at the base of the brain can all cause intense pain that is recognized as headache.” “…almost any type … of stretching stimulus to the blood vessels of the dura can cause headache.”
“Stimulation of pain receptors in the intracranial vault above the tentorium, including the upper tentorium surface itself, initiates impulses in the fifth nerve and, therefore, causes referred headache to the front half of the head in the area supplied by the fith cranial nerve.”
“…, pain impulses from beneath the tentorium enter the CNS mainly through the second cervical nerve, which also supplies the scalp behind the ear. Therefore, subtentorial pain stimuli cause ‘occipital headache’ referred to the posterior part of the head.”
Guyton, Arthur C., M.D.: Textbook of Medical Physiology. 6th Edition. W.B. Saunders, p.622, 1981.
“… tugging on the venous sinuses, damaging the tentorium, or stretching the dura at the base of the brain can all cause intense pain that is recognized as headache.” “…almost any type … of stretching stimulus to the blood vessels of the dura can cause headache.”
“Stimulation of pain receptors in the intracranial vault above the tentorium, including the upper tentorium surface itself, initiates impulses in the fifth nerve and, therefore, causes referred headache to the front half of the head in the area supplied by the fith cranial nerve.”
“…, pain impulses from beneath the tentorium enter the CNS mainly through the second cervical nerve, which also supplies the scalp behind the ear. Therefore, subtentorial pain stimuli cause ‘occipital headache’ referred to the posterior part of the head.”
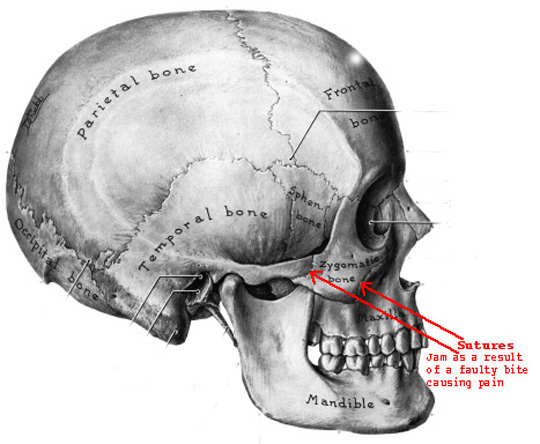
Figure 4 – Cranial Influences (above)
There are twenty two cranial bones (excluding the six ear ossicles) which function as a synchonized unit. A distortion to one affects the entire unit. The cranial dura is part of the dural tube which extends through the foramen magnum, attaches to the upper three cervical vertebrae and continues down to the second sacral tubercle where it attaches. Subluxations or fixations anywhere along its path will affect cranial motion. In addition, there are 136 muscles in the head and neck area. Muscle tension or spasm will influence cranial motion. Dental malocclusions in the form of hyper occlusion, deep overbite, crossbite (anterior or posterior), a narrow maxillary arch, faulty crowns or high cant of the maxillae on one side will all have influences on cranial motion.
The cause of the chronic facial pain was the inaccurate contact made by the posterior crowns. Improper contact resulted in jamming sutures between skull bones as well as tension placed on the dural membranes within the skull.
FREE PRESENTATION
Download the slides from Dr. Smith's presentation on the Dental Whole Body Connection in Ontario on October 25, 2024.
A comprehensive seminar to awaken you to the potential dangers of dental treatments.

STAY INFORMED
Big tech and mainstream media try to suppress the powerful information I have to share. Subscribe here to stay informed!