Since its introduction in 1983 by Darick Nordstrom, DDS, the ALF (Advanced Lightwire Functional) appliance has evolved into a sophisticated delivery system. The ALF paradigm evolved out of necessity. Doctor Nordstrom’s insight to the cranial component provided the basis for the ALF’s development. The biggest missing link in orthodontics has been the occlusal cranial connection. The ALF appliance System provides the vehicle for connecting these two components.
In 1995, this author introducted the diagnostic Occlusal Indicators to guide practitioners in the adjustment of the ALF. Four simple indicators, which are easily palpable on the patient’s skull quickly determine the pre-existing 3-dimensional distortions. By judiciously adjusting the ALF appliance the Cranial Indicators are manipulated, by the appliance, into a neutral position. The indicators tell the practitioner where the cranium is before, during and after treatment.
Completion of ALF treatment is achieved when the dental arches are adequately developed and removal of the ALF appliance allows all four of the cranial indicators to remain in balance (neural position). The process is simple, non-invasive, accurate and quickly carried out.
All truth passes through three stages. First, it is ridiculed. Second, it is violently opposed. Third, it is accepted as being self-evident. Arthur Schopenhauer
Eventhough great treatment outcomes have been witnessed with the ALF approach over the past thirthy three years, conventional orthodontists still violently oppose its acceptance. The reason is simple. Conventional orthodontists do not have the data base of knowlege to make the occlusal cranial connection. Once the dental community becomes enlightened, the third stage of truth, the acceptance phase will become self-evident.
Hidden in plain view. The occlusal cranial problems literally are staring orthodontic practitioners in the face but they cannot see it. A perfect example was my patient Ian, a 29 year-old who was a victim of four bicuspid amputation and retraction orthodontics carried out by an orthodontist who had a masters degree in orthodontics. For ten years Ian traveled the globe looking for answers to his chronic neck, low back pain overlaid with fatigue and loss of his
athletic ability and loss of mental clarity at age fourteen. I was the fourth orthodontist to evaluate his case. Upon viewing his maxillary study model, it became clear that his maxillae was compressed and rotated counter-clockwise by faulty orthodontic mechanics. Not knowing the cranial component of orthodontic treatment was the reason for this patient suffering for ten years and untold thousands of pounds spent seeking a solution.
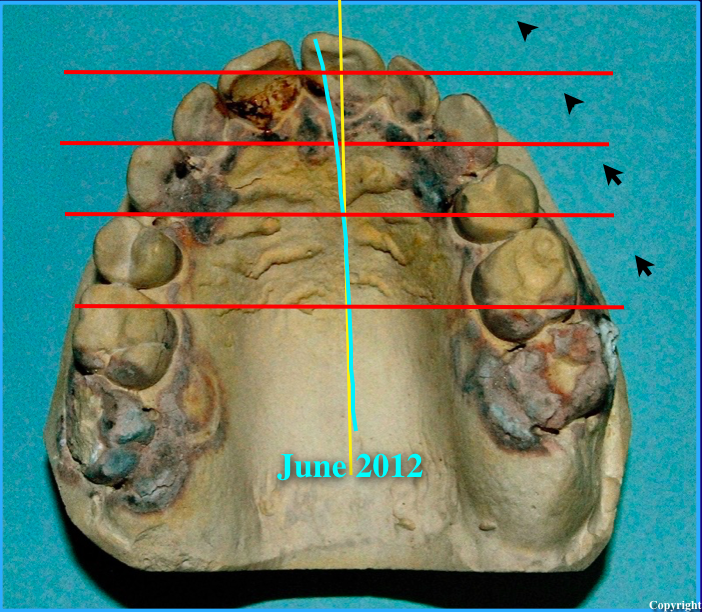
It becomes obvious once one views the horizontal misalignment of the right and left segments of the maxillary teeth. Faulty orthodontic mechanics literally rotated Ian’s maxillae in a counter- clockwise direction. This distortion put a twist into Ian’s dural tube, which extends down through the Foramen Magnum, attaches to the upper three cervical vertebrae and ends at the second sacral tubercle. Once the maxillae was rotated clockwise back to a neutral position, the dural torque was removed and Ian’s 10 years of chronic pain resolved. In addition to correcting the maxillary distortion, the maxillary anterior teeth had to be brought forward to allow the mandible to advance and the posterior teeth had to be erupted to decompress the spinal vertebrae. The process took three years to complete. Ian’s case could not have been corrected without the use of the Cranial Indicator System to guide the ALF and orthodontic adjustments.

The maxillary ALF appliance treats the maxillae as a single unit. Use of Class III elastics on the right and Class II elastics on the left enabled correction of the counter-clockwise distortion. The ALF also permits correction of the other cranial distions during the derotation process.
Conventional orthodontic brackets were used to complete the case. Use of the Cranial Indicators was critical in determining the correct force the elastics were exerting and when the correction was complete. There is no radiographic measurement that can give you the answer.

Since the maxillae represents the anterior two-thirds of the base of the human skull it must be balanced transversely and sagittaly and expanded and shaped to also provide balance to the intra cranal membrane system. Establishing a crooked maxillae sets the body up for spinal, pelvic, and sacral compensatory distortions. Without a level foundation, building the mandibular arch to a distorted upper is a prescription for diaster. Resolving TMJ problems also requires the temporal bones to be balanced. There is no way TMJ problems can be corrected with just an appliance without first correcting the door frame, the temporal bone. The condyles, disc, muscles and ligments all depend on balanced glenoid fossae, which are located in the temporal bones.

Once the foundation, maxillae, is established then the mandibular arch must be developed to fit into it. Since the occlusion is the self-correcting mechanism for balancing the cranial complex, having a balanced occlusal cranial relationship insures the stability of the spine, pelvis, and sacrum and health of the patient.


Embriologically the anterior teeth develop from the neural tube, which gives rise to the sympathetic nervous system. The posterior teeth develop from the neural crest cells of the brain, which give origin to the parasympathetic nervous system. Having a balanced occlusion
provides more than a pretty smile. It is paramount to balancing the autonomic nervous system and all its associated structures. This aspect is the connection to specific vertebrae, muscles, ligaments, and organs of the body.

Retreating four bicuspid amputation and retracted orthodontic cases are one of the most challenging exercises in orthodontics; however, using the Cranial Indicator Diagnostic System makes the process easier and helps insure a more successful out come. What other diagnostic system available to day gives the orthodontist the answer?

Curriculum Vitae
Doctor Gerald H. Smith is a recognized international authority on craniomandibular somatic disorders with a focus on resolving chronic pain. He is the author of a landmark textbook, Cranial-Dental-Sacral Complex and the first researcher in the world to radiographically document cranial bone movement by means of the Dental Orthogonal Radiographic Analysis System, which he developed. Doctor Smith also developed and patented the worlds first cranial motion precision attachment to permit cranial motion in fixed bridgework that crosses the maxillary mid-line. Doctor Smith is also the originator of the Occlusal Cranial Balancing Technique, the worlds first occlusal system to balance cranial bone and spinal alignment. He has also contributed equally important books, Reversing Cancer, Headaches Aren’t Forever and Alternative Treatments For Conquering Chronic Pain. His latest book presents a major paradigm shift by integrating osteopathic, chiropractic, dental, medical, physical therapy and nutritional concepts. Doctor Smith’s 46 plus years of clinical research has uncovered several of the major missing links for the cause of chronic pain and medical problems. He was an invited speaker at Walter Reed Army Medical Hospital, Yonsi Memorial Hospital in Seoul Korea, Holistic Medical Association and other prestigious meetings. He was a past president and editor of the Holistic Dental Association, and past president of the Pennsylvania Craniomandibular Society. He has a specialty practice in chronic pain, nutrition and dental orthopedics/orthodontics in Langhorne, Pennsylvania and Toronto, ONT.
